The Hidden Costs of Untrained Dental Assistants
Article by Julian L. Milian, CEO/Founder
Smart Medical Ventures
An untrained dental assistant does not just slow down one procedure. The wrong training gaps can quietly drain doctor time, create clinical stress, increase retakes and remakes, and weaken the entire flow of the practice.
The problem does not always look expensive at first
Most dentists do not feel the cost of an untrained dental assistant as one big event.
It usually shows up in smaller moments.
The tray is missing something.
The room is not fully ready.
The assistant does not anticipate the next step.
The suction is poorly positioned.
The doctor has to pause and explain.
A radiograph needs to be retaken.
A material is mixed too early or too late.
The turnover is slow.
The next patient is waiting.
None of these moments may seem catastrophic by themselves. But in a busy dental practice, repeated small delays become a serious production problem.
That is the hidden cost of an untrained dental assistant.
It is not only payroll. It is lost time, broken flow, doctor fatigue, patient frustration, staff stress, and rework that should have been prevented before the assistant ever reached the chair.
Most assistant problems are really readiness problems
When a new dental assistant struggles, the easiest assumption is that the person is not motivated, not focused, or not a good fit.
Sometimes that is true.
But often, the real problem is simpler: the assistant was never trained to perform inside real clinical flow.
There is a difference between knowing the name of an instrument and knowing when the doctor will need it.
There is a difference between passing a course and being able to keep a room moving.
There is a difference between watching a procedure and understanding the sequence, the timing, the risks, and the correction points.
A dental practice does not need assistants who only recognize terms. It needs assistants who can support production, protect clinical rhythm, and reduce unnecessary interruptions.
That requires clinical readiness.
The doctor pays for weak training with time
In a busy practice, the doctor’s time is the most valuable resource in the room.
When the assistant is not ready, the doctor becomes the backup trainer, the quality control system, the flow manager, and sometimes the assistant.
That creates a predictable pattern:
The doctor asks for an instrument that should have already been ready.
The doctor stops to correct suction or isolation.
The doctor explains a sequence during the procedure.
The doctor waits for materials.
The doctor repeats the same correction later in the day.
The doctor leaves the room already behind.
This does not just create frustration. It compresses the schedule.
When enough small breakdowns happen, the entire practice starts to feel rushed. Hygiene checks get squeezed. Treatment rooms fall behind. Patients wait longer. The team feels pressure. The doctor carries the clinical burden that should have been shared.
An untrained assistant does not just make the doctor work harder. An untrained assistant makes the entire day less efficient.
The most expensive errors are often the routine ones
The highest-cost assistant mistakes are usually not dramatic. They are common, repeated, and preventable.
1. Incomplete room and tray preparation
When the room is not ready, the procedure starts with friction. The doctor notices what is missing, the assistant leaves to find it, and the patient watches the team scramble.
That damages flow and confidence.
2. Weak instrument anticipation
A good assistant does not simply hand instruments when asked. A trained assistant understands sequence. They know what is likely coming next and prepare before the doctor has to say it.
Poor anticipation slows dentistry down.
3. Poor isolation and moisture control
Isolation is not a small skill. Weak suction, poor retraction, and moisture problems can affect visibility, efficiency, and the quality of restorative procedures.
The doctor feels this immediately.
4. Radiography positioning errors
Radiograph retakes waste time, frustrate patients, and interrupt the schedule. A student or new hire who cannot recognize positioning errors before exposure creates repeated inefficiency.
5. Slow or inconsistent turnover
Turnover problems do not stay in one room. They affect the next patient, the next provider, and the next scheduled procedure.
One slow turnover can push the whole column behind.
6. Material timing mistakes
Dental materials require timing, sequence, and attention. Mixing too early, too late, or incorrectly can waste product and delay the procedure.
7. Poor visibility support
Suction and retraction are not passive tasks. They are active clinical support skills. When visibility is poor, the doctor works harder, slows down, and becomes physically fatigued faster.
8. Weak documentation and handoff habits
Incomplete notes, unclear handoffs, and missed details create downstream problems for billing, scheduling, treatment planning, and team communication.
9. Failure to recognize errors early
This is one of the biggest differences between a trained assistant and an untrained one. A weak assistant may know that something went wrong after the doctor points it out. A stronger assistant learns to recognize the error pattern earlier and correct it faster.
That is where real readiness begins.
The Hidden $25,000–$100,000 Cost of an Untrained Dental Assistant in a Busy Practice
The ADA reports average 2025 gross billings per general practitioner in private practice at $965,660. If you model that over 200 clinical days and 7 productive clinical hours per day, that equals roughly $690 in gross billings per clinical hour. Even using a more conservative $500/hour production value, small daily assistant errors become very expensive fast.
The BLS lists median dental assistant pay at $22.74/hour, which helps make the contrast clear: the hidden cost is not just the assistant’s wage. The larger cost is the doctor time, chair time, schedule compression, and production flow being affected.
Here is the simple math:
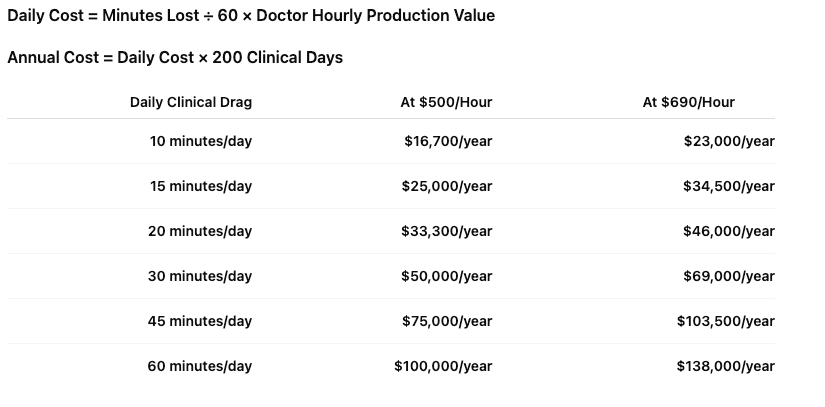
That means a practice does not need a major staffing disaster to lose money.
A few repeated breakdowns per day can create a $25,000 to $100,000 annual production drag.
Not because the assistant is a bad person.
Because the assistant was never trained, validated, and hardened for real clinical flow.
How Small Assistant Errors Turn Into Real Money
1. Incomplete room and tray preparation
If the doctor loses just 5 minutes per procedure because the room is not fully ready, and that happens 4 times in a day, the practice has lost 20 minutes of clinical flow.
That is approximately:
- $167/day at $500/hour
- $230/day at $690/hour
- $33,300 to $46,000/year over 200 clinical days
The missing item may look small.
The repeated interruption is not.
2. Weak instrument anticipation
When the doctor has to repeatedly ask for instruments, pause, redirect, and wait, the assistant is no longer protecting production flow.
Even 10 minutes per day of broken chairside rhythm can equal:
- $16,700/year at $500/hour
- $23,000/year at $690/hour
This is why anticipation is not a “nice to have” skill.
It is a production skill.
3. Poor isolation and moisture control
Poor isolation does not only frustrate the doctor. It can slow restorative dentistry, increase procedure time, and create quality risk.
If weak isolation adds 15 minutes to a restorative appointment, that single appointment may create a production drag of:
- $125 at $500/hour
- $173 at $690/hour
If that happens several times per week, it becomes a real business problem.
4. Radiography retakes
Radiography retakes are one of the clearest examples of hidden assistant cost.
A retake does not only use a few extra minutes. It interrupts patient flow, adds frustration, and pulls attention away from the schedule.
If positioning errors and retakes create only 10 minutes per day of wasted time, that equals approximately:
- $16,700/year at $500/hour
- $23,000/year at $690/hour
In a high-volume office, the number can be much higher.
5. Slow turnover
Slow turnover compresses the entire schedule.
If turnover delays create 20 minutes of lost flow per day, the annual cost can be:
- $33,300/year at $500/hour
- $46,000/year at $690/hour
The practice may not call it “lost production.”
It may call it running late, stressed staff, rushed hygiene checks, irritated patients, or the doctor staying late.
But the cost is still there.
6. Material timing mistakes
Material errors create waste, delays, and frustration.
If a material mistake adds 10 to 15 minutes to a procedure, that single error may cost the practice approximately:
- $83 to $125 at $500/hour
- $115 to $173 at $690/hour
The material itself may only cost a few dollars.
The clinical time costs much more.
7. Poor suction, retraction, and visibility support
Poor visibility makes the doctor work harder.
That can slow treatment, increase fatigue, and break the rhythm of the appointment.
If poor chairside support creates just 15 minutes per day of drag, that equals:
- $25,000/year at $500/hour
- $34,500/year at $690/hour
That is why suction and retraction are not basic tasks.
They are clinical flow skills.
8. Weak documentation and handoff habits
Poor documentation may not always cost money immediately, but it creates downstream risk.
Missed notes, unclear handoffs, incomplete treatment details, and billing confusion can create administrative rework and team frustration.
Even if the doctor is not directly involved, the practice is still paying for repeated correction.
9. Failure to recognize and correct errors early
This is one of the most expensive training gaps.
A weak assistant waits for the doctor to catch the problem.
A stronger assistant recognizes the error pattern earlier.
That difference matters.
If an assistant prevents even one 30-minute delay, remake, or avoidable schedule disruption per week, that can protect:
- $12,500/year at $500/hour
- $17,250/year at $690/hour
That is the value of clinical readiness.
That means a practice does not need a major staffing disaster to lose money.
A few repeated breakdowns per day can create a $25,000 to $100,000 annual production drag.
Not because the assistant is a bad person.
Because the assistant was never trained, validated, and hardened for real clinical flow.
How Small Assistant Errors Turn Into Real Money
1. Incomplete room and tray preparation
If the doctor loses just 5 minutes per procedure because the room is not fully ready, and that happens 4 times in a day, the practice has lost 20 minutes of clinical flow.
That is approximately:
- $167/day at $500/hour
- $230/day at $690/hour
- $33,300 to $46,000/year over 200 clinical days
The missing item may look small.
The repeated interruption is not.
2. Weak instrument anticipation
When the doctor has to repeatedly ask for instruments, pause, redirect, and wait, the assistant is no longer protecting production flow.
Even 10 minutes per day of broken chairside rhythm can equal:
- $16,700/year at $500/hour
- $23,000/year at $690/hour
This is why anticipation is not a “nice to have” skill.
It is a production skill.
3. Poor isolation and moisture control
Poor isolation does not only frustrate the doctor. It can slow restorative dentistry, increase procedure time, and create quality risk.
If weak isolation adds 15 minutes to a restorative appointment, that single appointment may create a production drag of:
- $125 at $500/hour
- $173 at $690/hour
If that happens several times per week, it becomes a real business problem.
4. Radiography retakes
Radiography retakes are one of the clearest examples of hidden assistant cost.
A retake does not only use a few extra minutes. It interrupts patient flow, adds frustration, and pulls attention away from the schedule.
If positioning errors and retakes create only 10 minutes per day of wasted time, that equals approximately:
- $16,700/year at $500/hour
- $23,000/year at $690/hour
In a high-volume office, the number can be much higher.
5. Slow turnover
Slow turnover compresses the entire schedule.
If turnover delays create 20 minutes of lost flow per day, the annual cost can be:
- $33,300/year at $500/hour
- $46,000/year at $690/hour
The practice may not call it “lost production.”
It may call it running late, stressed staff, rushed hygiene checks, irritated patients, or the doctor staying late.
But the cost is still there.
6. Material timing mistakes
Material errors create waste, delays, and frustration.
If a material mistake adds 10 to 15 minutes to a procedure, that single error may cost the practice approximately:
- $83 to $125 at $500/hour
- $115 to $173 at $690/hour
The material itself may only cost a few dollars.
The clinical time costs much more.
7. Poor suction, retraction, and visibility support
Poor visibility makes the doctor work harder.
That can slow treatment, increase fatigue, and break the rhythm of the appointment.
If poor chairside support creates just 15 minutes per day of drag, that equals:
- $25,000/year at $500/hour
- $34,500/year at $690/hour
That is why suction and retraction are not basic tasks.
They are clinical flow skills.
8. Weak documentation and handoff habits
Poor documentation may not always cost money immediately, but it creates downstream risk.
Missed notes, unclear handoffs, incomplete treatment details, and billing confusion can create administrative rework and team frustration.
Even if the doctor is not directly involved, the practice is still paying for repeated correction.
9. Failure to recognize and correct errors early
This is one of the most expensive training gaps.
A weak assistant waits for the doctor to catch the problem.
A stronger assistant recognizes the error pattern earlier.
That difference matters.
If an assistant prevents even one 30-minute delay, remake, or avoidable schedule disruption per week, that can protect:
- $12,500/year at $500/hour
- $17,250/year at $690/hour
That is the value of clinical readiness.
Untrained assistants also affect team morale
A weak assistant does not only impact the doctor.
Other team members feel it too.
The front desk hears patient frustration.
The hygienists feel the schedule pressure.
Other assistants have to cover gaps.
The office manager deals with complaints and turnover.
The doctor becomes more impatient because the same mistakes keep repeating.
Over time, the team stops trusting the training process.
That is when practices start saying things like:
“We just can’t find good assistants.”
“New hires are not what they used to be.”
“We have to train everyone from scratch.”
“No one comes out of school ready.”
“It is easier to do it myself.”
Those statements usually point to the same deeper issue: the practice does not have a reliable readiness standard.
Shadowing is not enough
Many practices try to solve the problem by having new assistants shadow experienced staff.
Shadowing can help with exposure. But shadowing is not a training system.
Watching someone set up a room does not prove the new assistant can do it independently.
Watching suction does not prove the assistant understands visibility, retraction, moisture control, and positioning.
Watching a radiograph does not prove the assistant can recognize an error before the image is taken.
Watching a procedure does not prove the assistant can support the sequence under real time pressure.
A strong practice needs more than exposure. It needs structure, repetition, correction, and validation.
That is the gap Clinical Ready™ was built to address.
Clinical Ready™ focuses on real practice performance
Clinical Ready™ is built around a simple idea:
Dental assistants should be trained for the way dentistry actually moves inside the practice.
That means students and new assistants need more than academic familiarity. They need practical readiness in the areas that affect daily flow:
Room preparation.
Tray setup.
Instrument identification.
Four-handed flow.
Isolation.
Moisture control.
Radiography support.
Turnover.
Infection control.
Material timing.
Documentation.
Error recognition.
Externship readiness.
Traditional training often moves students through a curriculum by topic. Clinical Ready™ is different because it focuses on whether the assistant can perform the skill in a way that supports the practice.
The goal is not to produce a student who can say, “I learned that.”
The goal is to produce a student who can show, “I can do that correctly, in sequence, under a standard.”
The hidden cost becomes visible when you measure the right things
Most practices do not track the cost of assistant readiness gaps. But they feel them every day.
A dentist should pay attention to questions like:
How often does the doctor have to stop and correct basic assistant tasks?
How often are radiographs retaken because of positioning errors?
How often are rooms not fully ready before seating?
How often does turnover push the schedule behind?
How often are materials wasted because of timing or mixing mistakes?
How often does the doctor repeat the same correction to the same team member?
How often do new hires leave before becoming productive?
These are not just training issues.
They are business issues.
A practice can lose thousands of dollars in time, inefficiency, remakes, retakes, stress, and turnover without ever seeing a single line item called “untrained assistant cost.”
That is why assistant readiness deserves the same attention as marketing, scheduling, case acceptance, and production.
The better question: are you hiring assistants, or building them?
The dental assistant shortage has forced many practices into a reactive hiring cycle.
They post a job.
They interview.
They hire quickly.
They train under pressure.
They hope the person works out.
Then they repeat the process when the person leaves or fails to meet expectations.
That cycle is expensive.
The stronger strategy is to build a workforce pipeline.
That is where a practice-based dental assisting school becomes powerful. Instead of waiting for the labor market to send better assistants, the practice creates a training pathway built around its own standards.
With the right system, a dental practice can do more than hire assistants.
It can train them. Validate them. Build them. And create a local talent pipeline that supports both the practice and the community.
The Real Cost May Be $25,000 to $100,000 Per Year
For many practices, the cost of an untrained dental assistant is not one dramatic mistake.
It is the daily accumulation of small breakdowns:
A few minutes looking for instruments.
A few minutes correcting suction.
A few minutes retaking radiographs.
A few minutes waiting on turnover.
A few minutes correcting materials.
A few minutes re-explaining the same task.
At only 15 minutes per day, the annual drag can reach $25,000 to $34,500.
At 30 minutes per day, it can reach $50,000 to $69,000.
At 45 to 60 minutes per day, the hidden drag can climb from $75,000 to more than $138,000 in gross production opportunity.
That is why assistant training is not just a staffing issue.
It is a production issue.
Final thought
The cost of an untrained dental assistant is not limited to wages.
It shows up in doctor interruptions, slower procedures, repeated corrections, poor flow, patient delays, radiograph retakes, material errors, team frustration, and preventable turnover.
A busy practice cannot afford to keep absorbing those costs.
The solution is not just hiring more people.
The solution is building better readiness before the assistant is trusted to carry the clinical load.
That is the purpose of Clinical Ready™.